Maturing Millennials in an Aging Society
End-of-life care encompasses the special support and attention given to an individual during the period leading up to death (National Institute of Health 2014). Though this life stage may appear too distant for millennials to appreciate, given their relative youth, many millennials already serve as informal caregivers[i]. Approximately one in every four caregivers in the United States are between 18 and 34 (The Editors 2015).
While millennials may not yet consider long-term care for themselves, many may join the ‘informal care’ workforce to offset the costs of care for their elderly parents or grandparents. A 2015 Rand study found that the opportunity cost of informal care (cash not earned by the caregiver due to lost time) is $522 billion annually in the U.S. (Chari, Amalavoyal, Engberg, John, Ray, Kristin, Mehrotra, 2015). Forty-seven percent of informal caregivers are older children or grandchildren, otherwise known as “working-age adults” (Chari, Amalavoyal, Engberg, John, Ray, Kristin, Mehrotra, 2015). If the informal services were replaced by professional nursing staff service, the cost of replacement would be $642 billion annually (Chari, Amalavoyal, Engberg, John, Ray, Kristin, Mehrotra, 2015).
To understand the relationship between millennials and the challenges posed by current and future end-of-life care responsibilities and demands, we examined the following research questions from public health and human rights perspectives:
a. What are the chasms separating end-of-life care theory (laws, regulations, policies, and guidelines) and practice (the application of policy at the service level) in the United States, and how do they impact maturing millennials?
b. What are the actions needed to protect both current and future patients’ right to end-of-life care, in a resource-scarce era of a rapidly aging society?
Methods and Materials
We conducted a content analysis of end-of-life care by comparing theory to practice. More specifically, we compared laws, regulations, and guidelines to their policy application at the service level. We first abstracted the primary terminologies from sources including the Federal Register, Code of Federal Regulations, state law, regulatory bodies, professional trade organizations and other concerned entities. Second, we explored the practice of end-of-life care by examining terminologies from scientific articles, reports, guideline recommendations, surveys, newspaper articles, and online information. To better understand the translation and evolution of the regulatory intent to practice, we conducted policy interviews with experts from relevant trade organizations and professional institutions for cross verification of data.
To examine the theory and practice regarding end-of-life care, aiming to investigate solutions to improve the current public health policy, we used a combination of public health and human rights-based approaches, which are normally separated by professional boundaries.
The public health approach focuses on prevention, population-based perspectives, evidence-based principals, and the impact of social, structural, and environmental determinants of health. This approach also focuses on the elimination of health disparities, which are vulnerabilities caused by poverty, discrimination, health illiteracy and inadequate education (Neff, 2014). A public health approach aims to increase community involvement by including health promotion activities that focus on education and empowerment, for individuals and their overall communities (Libby Sallnow et al. 2016, Betty R Ferrell and Coyle 2010).
We also used a human rights-based approach that aims to realize human rights by improving policies and programs. The approach has been developed and widely used by the United Nations (UN) and its member countries (United Nations HRBA, 2016). We employed the following essential elements of a human rights-based approach to our analysis of end-of-life care: availability accessibility, acceptability, and quality of health care; universality (non-discrimination); and accountability of the government and health care providers (UN Development Group 2011).
While we recognize the importance of tangential issues, such as end-of-life care for children and young adults, as well as physician-assisted suicide laws, this article does not include these topics due to space limitation.
Findings
Analysis: Theory and Practice in End-of-life Care
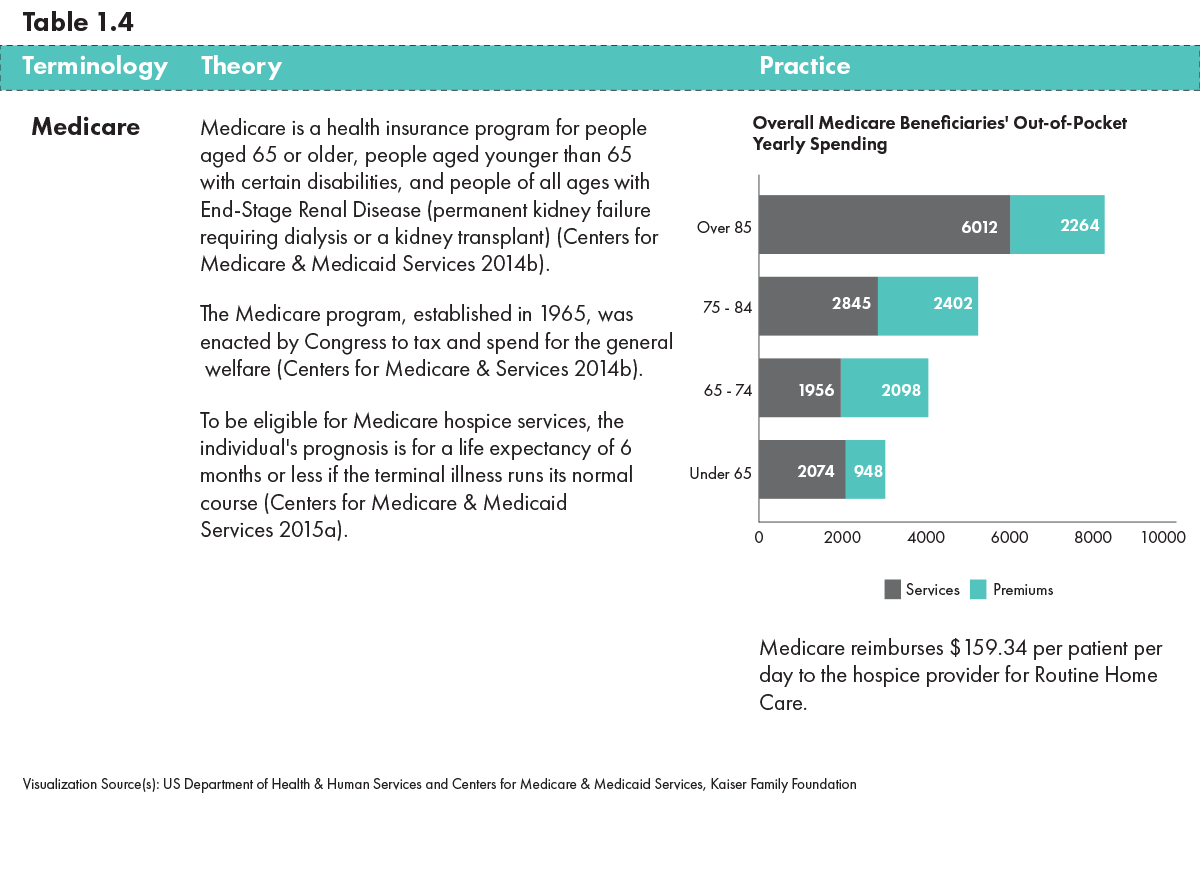
Our combined public health and human rights-based approach to end-of-life care presented both theoretical and practical accomplishments and concerns. We focused on specific populations, universality of care, and opportunity for prevention. We identified ten primary areas related to our research questions: end-of-life care, palliative care, hospice care, Medicare, long-term care, advance directives, well-being, spirituality, bereavement counseling, and dignity. The definitions and the synthesis of our analysis of the primary terminologies, theory, and practice in end-of-life care, are discussed and are presented in the Tables.